









































































































































I. Thuhmahruai
Distal humerus hi medial leh lateral column atanga siam a ni a, chung zingah chuan epicondyles leh condyles te pawh a tel a ni.
II. Surgery tih dan tur
Distal humerus fracture hi direct trauma (eg, tlu) emaw indirect force (eg, twisting emaw muscle pull) vang a ni.
III. Post-op Rehabilitation neih a ni
AO classification hian distal humerus fracture hi chi thum ah a then a, chungte chu A , B , leh C te an ni.
IV. Zirna Results
Surgical treatment hian AO principles a zawm a: taksa peng hrang hrang tihtlem, stable fixation, leh early rehabilitation.
V. Case Report chungchang
Locking plate hian biomechanical stability tha zawk a pe a, a bik takin osteoporotic bone-ah chuan.
VI. Sawiho
CZMEDITECH hian model pathum a pe a, chungte chu extraarticular (01.1107), lateral (5100-17), leh medial (5100-18) plate te an ni.
VII. Tawpna
Surgical treatment hian AO principles a zawm a: taksa peng hrang hrang tihtlem, stable fixation, leh early rehabilitation.
Distal tibial fracture hi a awm fo a, traditional treatment-ah pawh hian tihkhawtlai a awm
Distal tibial fracture hi ke hnuai lam ruh tliak chi khat a ni. Traditional treatment locking plate leh antegrade intramedullary nail te hian an that lohna an nei vek a. Locking plate hian operation hnua infection emaw soft tissue necrosis emaw a thlen thei a, dam rei theihna a siam thei a; antegrade nails hi a invasive tlem hle nachungin, khup ruh a tichhia thei a, natna a thlen thei a, fixation tha lo emaw malalignment emaw hlauhawmna a keng tel a, chu chuan dam lehna a tikhawlo thei a ni.
Locking plate te chu:
Soft tissue chhiatna nasa tak, infection rate sang, dam rei tak
Antegrade nail te chu:
Khup ruh hliam, fixation tha tawk lo, malalignment awm awlsam
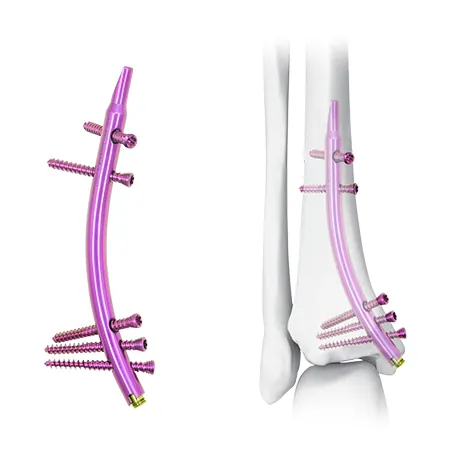
A chinfel dan thar: Distal Tibial Nail (DTN) tih a ni.
Treatment option thar—Distal Tibial Nail (DTN)—chuan a retrograde design danglam tak hmangin distal tibial fractures enkawl dan tur thlirna thar a pe a ni.
Retrograde insertion design hian kalphung thar a pe a ni

Damlo awmna tur leh tihtlem tura inbuatsaihna
Damlo chu supine position-ah dah a ni. Displaced fractures chu kut hmanga tihtlem theih a ni tur a ni; a tul chuan DTN dah hmain reduction forceps hmangin tanpui rawh. Fibular fracture a awm chuan fibular alignment dik tak chuan tibial reduction a pui thei a ni. Fibular shaft fracture hi intramedullary nail hmangin a stabilize thei bawk. Ankle chhehvela fracture awm tan chuan malalignment awm loh nan tibial reduction hmaah anatomical reduction leh fibula fixation a awm tur a ni. Open fracture-ah chuan external fixation awm tawhah chuan nail chu fixator enkawl chungin reduction neih theih nan dah theih a ni.
Supine position, a tul chuan reduction forceps hmang rawh
Tibial reduction dik tak neih theih nan fibular fracture management hi dah pawimawh hmasa rawh
Medial malleolus tip-ah 2–3 cm a sei incision siamin superficial deltoid ligament chu a lang chhuak thin. Guide pin chu malleolus tip (Fig. 2a)-ah emaw, a medial-ah emaw, articular surface atanga 4–5 mm-a hlaah dah a ni. Lateral view-ah chuan intercondylar groove kaltlangin insertion a awm (Fig. 2b), posterior tibialis muscle tihchhiat a awm loh nan. Superficial deltoid ligament chu then hran la, chutah chuan reamer hmangin medullary canal chu metaphyseal region thlengin ti lian rawh (Fig. 2c). Nail dah turin proximal medial cortex bula cancellous bone chu la chhuak rawh (Fig. 2d). DTN size finfiah nan trial nail dah la (Fig. 2e). Iatrogenic medial malleolar fracture ven nan hammer emaw, twisting tam lutuk emaw tih loh tur. Distal screw te chu ankle joint emaw fracture site emaw a luh loh nan nail depth chu siamrem rawh. Fixation hi proximally leh distally-a interlocking screw hmanga tih theih a ni.
Incision na hmun: 1.1.
Medial malleolus tip-ah longitudinal cut a ni
Guide pin awmna tur: 1.1.
Joint surface atanga 4–5 mm a hlaah a awm
Reaming & trial nail hmanga siam:
Metaphysis thlengin ream la, nail size chu confirm rawh
Nail dah dan: 1.1.
Hammering pumpelh la, joint ven nan depth siamrem rawh
Fixation tih dan tur:
Screw inzawmkhawm chu proximally leh distally-ah a awm


DTN dah luh dan tur





Ankle joint mobility leh foot-to-floor contact nghal theih a ni postoperatively
Non-weight bearing for 4–6 weeks
Kar 8–12 inkarah full weight-bearing-ah hmasawnna, chutih rualin callus siam leh natna enfiah a niAnkle joint activity hi operation zawh nghal a ni
Kar 4–6 chhung chu rit phurh loh tur
Kar 8–12 chhungin full weight-bearing-ah zawi zawiin a inthlak thin
Damlo 10 enkawl zui a ni
Zirna pakhatah chuan damlo 10 an enfiah a (Table 1). Thla 3 post-op-ah chuan case 7 an dam tawh a; damlo zawng zawng hian thla 6 chhungin damna an nei vek a ni. Varus leh recurvatum deformities pakhat ve ve a awm a. Reduction hloh, infection, implant-related complications, iatrogenic injuries emaw hmuh tur a awm lo (Table 2).
Thla 3 chhungin hri kai enkawl dam mi 7; thla 6 chhungin an dam vek
A pianphung na lo 2 (varus 1, recurvatum 1) .
Infection, implant complication, emaw reduction loss emaw a awm lo


Kum 69 mi mipa damlo a ni
Fracture chi hrang hrang: 1.1.
Transverse tibial fracture + fibular tihchhiat a ni
Harsatna awm thei: 1.1.
Soft tissue crush hliam a awm
Post-op-ah chuan:
Incision tenau 6 chauh, kum 1 chhungin a dam kim vek
Figure 3 & 4-ah hian:
Radiographic leh operation hnua dam lehna thlalak







DTN hman dan tur hriattirna
He zirchiannaah hian AO 43-A leh C1 fracture te; C2 pawh ngaihtuah a ni. DTNs hi 7 mm leh 8 mm a sei a awm a, hei hian proximal interlocking screw dahna tur a hril a ni. Articular surface atanga cm 2–9 a sangah fracture awm hi DTN fixation atan chuan candidate tha tak a ni. Indication te hi AO 42 fracture thlengin tihzauh theih a ni.
AO 43-A, C1-a hman theih tur chuan C2 leh 42-a tihzauh tum ang che
Joint surface atanga cm 2–9 a hlaa fracture awm tan chuan outcome tha ber
Biomechanical lama a dinhmun a nghet thei
Retrograde nail hian medial locking plate leh antegrade nail te aiin axial leh rotational stiffness a nei tha zawk a ni. Greenfield leh a thawhpuiten an sawi. biomechanical testing an nei a, DTN-a distal screw pahnih hman hian screw pathum nena khaikhin chuan compressive stiffness 60–70% leh torsional stiffness 90% a nei tih hmuhchhuah a ni. DTN hian load hnuaia fracture fragment movement a ti tlem hle. Thla 3 chhunga dam lo case 3 ah chuan factors te chu soft tissue chhiatna, medullary expansion, fracture location, leh osteoporosis te a ni. DTNs hi size pathum chauh a awm a, distal fixation chu screw pathum chauh a nih avangin wide canals emaw osteoporotic bone emaw-ah stability tling lo a pe thei a ni. Chutiang hunah chuan rit phurh hmasak hi fimkhur taka kalpui tur a ni.
Locking plate leh antegrade nail aiin a tha zawk
Fixation hmanraw tha ber: proximal screw 2 + distal screw 3
DTN hman thatna
Locking plate nena khaikhin chuan intramedullary nail hian soft tissue a tichhia tlem zawk a, a bik takin damlo tar leh high-energy trauma avanga soft tissue hliam na tak nei tan a tha hle. He zirchiannaah hian DTNs hi incision tenau paruk chauh hmanga dah a ni a, soft tissue complication a awm lo. He procedure hian khup flexion a ngai lo va, reduction loss hlauhawmna a ti tlem a, khup motion tlem (eg, knee arthritis emaw post-TKA) nei damlote tan pawh a tha hle.
Minimally invasive, tar leh high-energy trauma patient tan a tha hle
Knee flexion a ngai lo, khup mobility limited tan a tha
Surgical Risk leh fimkhur dan tur
Risk te chu posterior tibialis muscle hliam leh medial malleolar fracture te a ni. Medial malleolar fracture hi tension band wiring, plating, emaw pawn lam fixation hmanga enkawl theih a ni.
Fibular notch chhunga screw lut lo turin fimkhur a ngai. Positioning device hian DTN chu a rit lutuk avangin a hnunglam a tichhe thei a; screw pahnihna chu fibula lam hawi turin siamrem rawh (Fig. 4c).Harsatna awm thei: 1.1.
Posterior tibialis hliam, medial malleolar ruh tliak
Enkawltu:
Tension band, plating, emaw pawn lam fixator emaw a ni thei
Screw lam hawi leh positioning device rit zawng hi intraoperative attention a ngai a ni
Clinical lama tehkhin dan
Antegrade nail-a nonunion leh malalignment rate chu 0–25% leh 8.3–50% a ni a; locking plate atan chuan 0–17% leh 0–17% a ni. He zirchiannaah hian case zawng zawng hian union an nei vek a, 20% chauhvin deformity >5° an nei a, hei hi hmanlai method nena khaikhin theih a ni.Infection rates: superficial infection chu antegrade nail-ah 0–8.3% a ni a, locking plate-ah 0–23% a ni deep infection hi 0–23% leh 0–8.3% a ni. He zirchianna hian soft tissue complication a nei lo tih a report a, alternative pahnih hi a phak lo hle.Functional scores:
AOFAS score-ah hian antegrade nail-te chu: 86–88 (type A), 73 (type C); a khar theihna plate: 84–88 (type A) .
He zirchianna hian: AOFAS average: 92.6
EQ-5D-5L: Locking plate-te chu 0.62–0.76 a ni a; he zirchiannaah hian: 0.876
SAFE-Q (ke leh ke ruh damlo): 67–75; he zirchianna hi: 83–91.7 (Table 3) .
Union rate, deformity rate leh infection rate te hian hmanlai kalphung aiin a ti tha zawk a ni
Functional score (AOFAS, EQ-5D-5L, SAFE-Q) te hian result tha tak tak a nei a ni

A tawi zawngin, DTN hian locking plate leh antegrade intramedullary nails aiin a thatna a pe a, distal tibial fracture enkawlna atana solution tha tak a ni.
DTN hian invasiveness a nei tlem hle a, stability sang tak a nei a, a dam chak hle bawk
Traditional treatment aia hlu tak a ni a, tihlar tlak a ni

A rilru a buai em em a, a rilru a hah em em bawk a. Distal Humeral Extraarticular Locking Plate
Model: 01.1107 a ni


A rilru a buai em em a, a rilru a hah em em bawk a. Distal Lateral Humeral Locking Plate
Model: 5100-17 ah a awm

A rilru a buai em em a, a rilru a hah em em bawk a. Distal Medial Humeral Locking Plate
Model: 5100-18 ah a awm

