Rupture of the extensor tendon after volar plate fixation remains a major problem in the repair of distal radius fractures. The most commonly affected tendon is the extensor pollicis longus (EPL) tendon, as it is confined within the EPL groove. The reported incidence of EPL tendon rupture after volar plating is 0.29%–5.7%.
The risk of delayed EPL tendon rupture is increased in the presence of dorsal screw protrusion, injury from intraoperative direct drilling, and dorsal roof fragments, especially in island fractures of Lister's tubercle. Radiographic assessment of screw protrusion in distal radius fractures is difficult due to the complex geometry of the distal radius and the potential for comminuted dorsal fractures. The dorsal tangential view is the only possible intravital view of the dorsal radial cortex to obtain a reliable assessment of the distance between the screw tip and the dorsal cortex.
Techniques to avoid extensor tendon injury include the use of monocortical screws and avoidance of dorsal surface penetration; however, these techniques may reduce the mechanical stability of fracture repair. Therefore, bicortical fixation is sometimes required. To minimize the risk of extensor tendon injury, the primary goals of fracture fixation and stability must not be compromised.
New surgical techniques
We describe a novel technique to minimize the risk of EPL tendon rupture after volar plate fixation of distal radius fractures without shortening the screw length or removing dorsal roof fragments. Briefly, the technique involves opening the third compartment through a small dorsal incision.
If the screw had penetrated the dorsal cortex and protruded in the third compartment: we removed the EPL tendon from its groove and closed the compartment by sutured the retinaculum leaving the EPL tendon on the repaired retinaculum.
If the screw does not extend into the third compartment: we leave the EPL tendon in the third compartment. The indication for our technique is in patients with distal radius fractures treated with volar locking plates, fractures with dorso-parietal fragments or screws that may penetrate the dorsal cortex or damage the EPL tendon around the Lister's tubercle. In patients with distal radius fractures with dorsomedial fragments, we drill holes to penetrate the dorsal cortex and select screws of sufficient length to fix the unstable dorsomedial fragments.
Case sharing
We share a case in which the EPL tendon was removed from the third compartment due to protrusion of the screw in the third compartment during plate fixation of a comminuted distal radius fracture with dorsomedial fragments. We confirmed that the EPL tendon was intact 7 years postoperatively, although the screw was prominent in the third compartment.
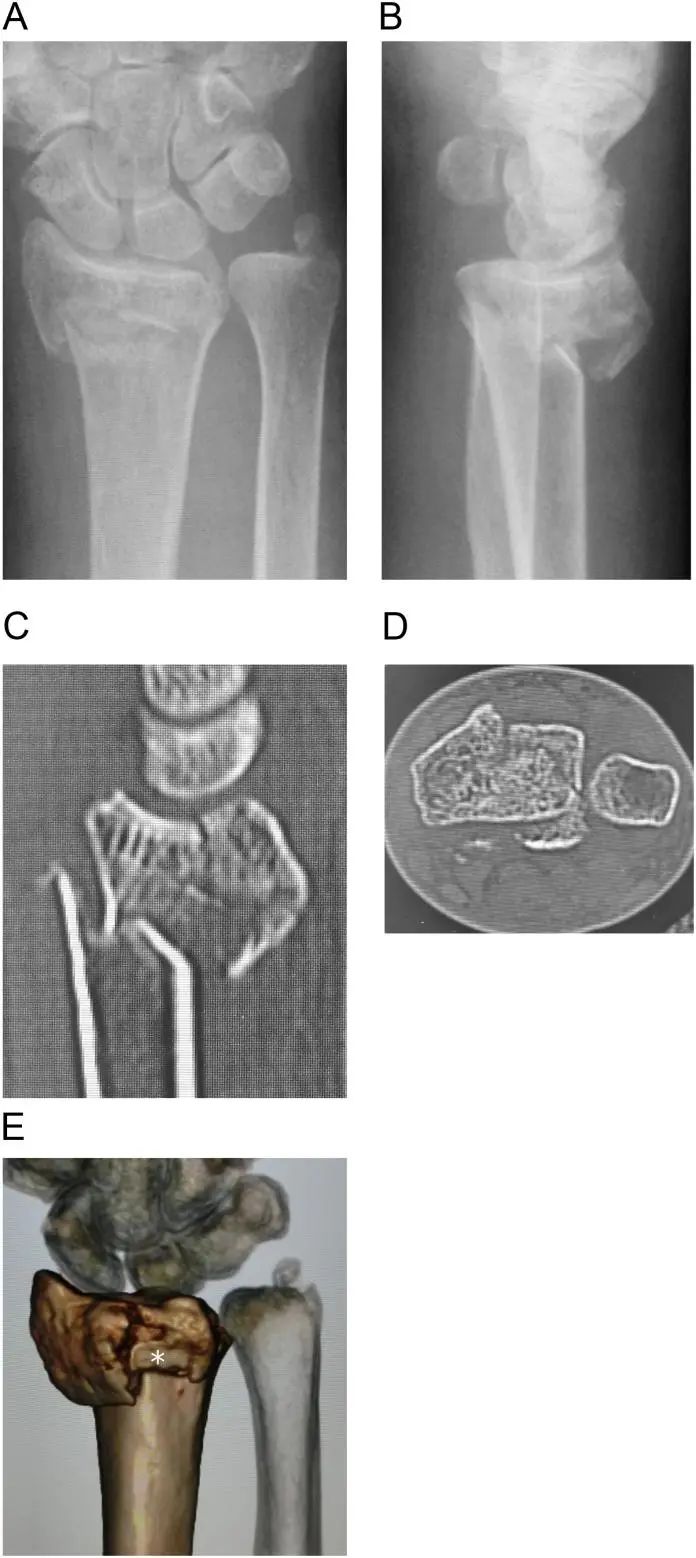
The case was a 67-year-old female with a diagnosis of an intra-articular unstable distal radius fracture with a right dorsal medial fracture (Figure 1A-E). No history of smoking, diabetes or alcohol consumption. Can walk without any walker.
![distal radius fracture]()
figure 1. Preoperative imaging showed a comminuted intra-articular fracture of the distal radius.
A and B: Preoperative X-rays,
C and D: sagittal and axial views of computed tomography images,
E: 3D computed tomography image. Dorsal medial lunate facet fragments and dorsal apical fragments (white asterisks) are visible.
Surgical technique
We treated this fracture system with a volar locking plate. Intraoperatively, we drilled through the dorsal cortex and selected a screw long enough to secure the dorsal cortex because the dorsomedial fragment was unstable (Figure 2).
Surgery was performed to open the third compartment after screw fixation.
Since the screw has penetrated the third compartment and protruded (Figure 3A), fully open the third compartment and move the EPL tendon out of its groove (Figure 3B).
The third compartment was then closed by suturing the retinaculum (Fig. 3C,D), and the EPL tendon was placed over the repaired retinaculum (Fig. 3 E).
After surgery, the patient went to the outpatient clinic of our hospital until the bone healed. The patient does not wish to remove the hardware.
Postoperative recovery
Seven years after the operation, the patient returned to the hospital for re-examination due to osteoporosis. The right hand is not disabled. X-ray image showing a healed fracture with dorsal protrusion of the distal locking screw. The patient's thumb was fully extended, and the EPL tendon had no obvious bowstring.
At our recommendation, the patient agreed to remove the hardware and examine the extensor tendons. Intraoperatively, we examined the EPL tendon through a dorsal incision and partially opened the third and fourth compartments.
The EPL tendon was located outside the third compartment in the same position as in the previous operation, and the tendon was not irritated.
We confirmed that the screw entered the third compartment when the extensor tendons of the fingers were retracted.
Finally, we fixed the support straps and removed the hardware. At the final evaluation 2 months after removal of the hardware, the patient was pain free and had full thumb extension.
Discuss
In our approach, after volar plate fixation of distal radius fractures, we partially opened the third compartment through an incision approximately 2 cm long ulnar to the tubercle of Lister. We directly identified the EPL tendon and the floor of the third extensor compartment by gently retracting the EPL tendon.
If the screw penetrated the dorsal cortex into the third compartment or had dorso-parietal debris, we did not perform intraoperative screw replacement or fragmentectomy, but completely opened the third compartment and removed the EPL tendon from its groove. We then closed the compartment by suturing the retinaculum while repositioning the EPL tendon on the third compartment.
If the screw did not extend into the third compartment, we left the EPL tendon in the partially opened third compartment.
Our surgical technique allows easy inspection of EPL tendon injuries with direct visualization in as little as an additional 10 minutes. If the EPL tendon is injured, it can be repaired directly. This procedure helps prevent secondary EPL tendon rupture after distal radial plate fixation. EPL tendon bowstring may occur, but it did not occur in our case.
In conclusion
We experienced a case in which the EPL tendon was intact 7 years postoperatively, although the screws used to fix the volar plate were prominent in the third compartment. Our surgical technique minimizes the risk of EPL tendon rupture after volar plate fixation for distal radius fractures.
How to Buy Orthopaedic Implants and Orthopaedic Instruments?
For CZMEDITECH, we have a very complete product line of orthopedic surgery implants and corresponding instruments, the products including spine implants, intramedullary nails, trauma plate, locking plate, cranial-maxillofacial, prosthesis, power tools, external fixators, arthroscopy, veterinary care and their supporting instrument sets.
In addition, we are committed to continuously developing new products and expanding product lines, so as to meet the surgical needs of more doctors and patients, and also make our company more competitive in the whole global orthopedic implants and instruments industry.
We export worldwide, so you can contact us at email address song@orthopedic-china.com for a free quote, or send a message on WhatsApp for a quick response +86-18112515727.
If want to know more information,click CZMEDITECH to find more details.