Views: 70 Author: Site Editor Publish Time: 2022-10-21 Origin: Site
Intramedullary tibial nailing: access and alignment, anterior knee pain
The surgical approach to intramedullary nailing of tibial fractures is important in order to insert the intramedullary nail through the correct entry point, to minimize damage to the intra-articular knee structures, and to achieve optimal fracture repositioning and proper nail entry.
The classic approaches for tibial stem fractures are the infrapatellar median or infrapatellar parapatellar approach. Although these approaches are indicated for mid-segment fractures, postoperative valgus, anterior, or combined deformities frequently occur in more proximal fractures.
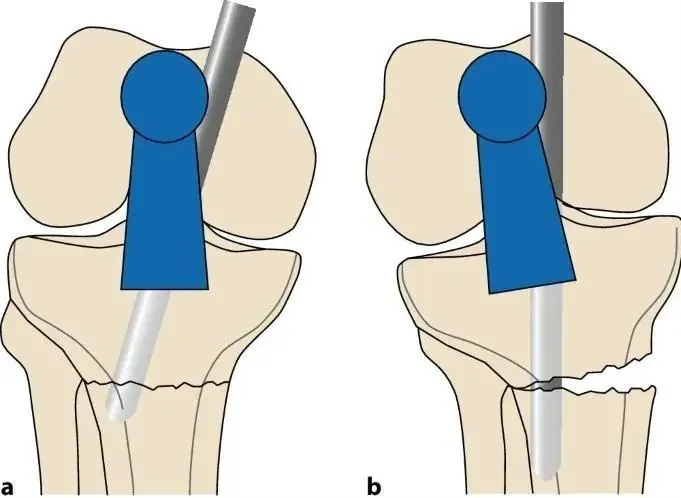
The main cause of malalignment in proximal tibial fractures is deformity caused by pulling of the quadriceps tendon during knee flexion and mechanical conflict between the nail tip and the posterior tibial cortex during implant insertion. The patella also prevents axial nail entry in the sagittal plane (Fig. 1a, b). Therefore, another common method of accessing the point is through a medial parapatellar incision, which leads to a slight medial to lateral nail insertion (Figs. 1c and 2). As the nail enters the intramedullary canal distal to the fracture, the proximal portion tilts into valgus (Figure 2). Finally, the resting tension of the anterior compartment muscles contributes slightly to the valgus (Figure 3).
Figure 1 a,b Using the conventional infrapatellar approach, the patella prevents axial entry of the nail, resulting in the common deformity of anterior apical sagittal alignment and valgus coronal alignment. c Using the parapatellar approach for intramedullary nail alignment.
Figure 2 Approaching the entry point through a medial parapatellar incision leads to a slightly medial to lateral nail insertion. As the nail enters the medullary canal distal to the fracture (a), the proximal portion tilts into valgus (b)
Figure 3 Resting tension in the anterior muscle compartment ( a ) produces a subtle ectopic arrangement ( b )
Pinning the tibia in a more extended position helps avoid complications associated with severe intraoperative knee flexion. the technique was described by Gelbke, Jakma et al. in 2010 and has become increasingly popular in recent years because pinning the tibia in an almost straight limb position simplifies fracture manipulation and repositioning. Fluoroscopy has become technically easier to perform. Fluoroscopy times for suprapatellar nailing have been reported to be significantly shorter than for infrapatellar nailing. In addition, the angle of nail insertion (in the sagittal plane) is more parallel to the longitudinal axis of the tibia in this approach than in the infrapatellar nail; this prevents mechanical conflict between the nail tip and the posterior cortex, thereby facilitating fracture reduction.
Postoperative anterior knee pain is a related problem. Anterior knee pain has been reported in 50-70% of fracture patients, with only 30% of patients experiencing pain relief after removal of the internal plant. It is estimated that scar formation associated with access to the patellar tendon and Hoffa fat pad is a potential source of postoperative knee pain. In addition, the suprapatellar approach avoids the traditional incision of the branch of the patellar branch of the saphenous nerve, thereby avoiding anterior knee numbness and sensory dullness (Figure 4). Passing the nail through the quadriceps tendon, thereby leaving the patellar tendon intact, appears to significantly reduce the rate of postoperative knee pain.
Due to the good results of proximal fractures, the indications in clinical practice have been extended to all fractures.
When should a suprapatellar intramedullary nail be used?
Advantages
Semi-extended knee position promotes fracture manipulation and repositioning by relaxing muscle strength and retention during nail insertion
Lower risk of postoperative dislocation of proximal, segmental and distal fractures compared to conventional techniques
Nailing operation is technically easier to perform
Nail insertion is feasible as a "single surgeon procedure"
Reduced fluoroscopy time
No damage to the patellar tendon and lower incidence of post-stapling anterior knee pain
Easier to perform in a multi-team procedure, as in multiple trauma
Indications
Extra-articular fracture of the proximal tibia (AO 41A type)
Simple comminuted fracture of the tibial diaphysis (AO 42A-C type)
In addition, we are committed to continuously developing new products and expanding product lines, so as to meet the surgical needs of more doctors and patients, and also make our company more competitive in the whole global orthopedic implants and instruments industry.
We export worldwide, so you can contact us at email address song@orthopedic-china.com for a free quote, or send a message on WhatsApp for a quick response +86-18112515727.
If want to know more information,click CZMEDITECHto find more details.
This website uses cookies and similar technologies (“cookies”). Subject to your consent, will use analytical cookies to track which content interests you, and marketing cookies to display interest-based advertising. We use third-party providers for these measures, who may also use the data for their own purposes.
You give your consent by clicking "Accept all" or by applying your individual settings. Your data may then also be processed in third countries outside the EU, such as the US, which do not have a corresponding level of data protection and where, in particular, access by local authorities may not be effectively prevented. You can revoke your consent with immediate effect at any time. If you click on "Reject all", only strictly necessary cookies will be used.